Childhood Multiple Endocrine Neoplasia (MEN) Syndromes Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Childhood Multiple Endocrine Neoplasia (MEN) Syndromes
Multiple endocrine neoplasia (MEN) syndromes are inherited disorders that affect the endocrine system.
The endocrine system is made up of glands and cells that make hormones and release them into the blood. MEN syndromes may cause hyperplasia (the growth of too many normal cells) or tumors that may be benign (not cancer) or malignant (cancer).
There are several types of MEN syndromes and each type may cause different conditions or cancers.
The two main types of MEN syndromes are MEN1 and MEN2. MEN2 syndrome has two subgroups: MEN2A syndrome and MEN2B syndrome. MEN2A syndrome includes familial medullary thyroid cancer.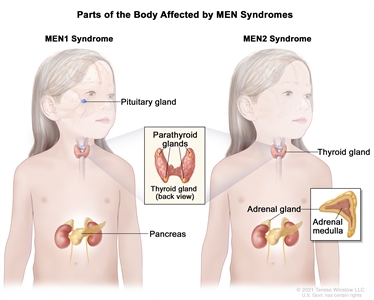
Multiple endocrine neoplasia (MEN) syndromes are rare, inherited disorders that affect the endocrine glands or organs. There are several types of MEN syndromes, and each type may cause different conditions or cancers. The two main types of MEN syndromes are MEN1 and MEN2. MEN1 syndrome usually causes tumors in the pituitary gland, parathyroid gland, or pancreas. MEN2 syndrome usually causes tumors in the thyroid gland, parathyroid gland, or adrenal gland. The tumors may be benign (not cancer) or malignant (cancer).
MEN1 syndrome usually causes tumors in the parathyroid gland, pituitary gland, or islet cells of the pancreas.
A diagnosis of MEN1 syndrome is made when tumors are found in two of the following glands or organs: parathyroid gland, pituitary gland, or islet cells in the pancreas. These tumors may make extra hormones and cause certain signs or symptoms of disease. The signs and symptoms depend on the type of hormone made by the tumor. MEN1 syndrome is also called Wermer syndrome.
The prognosis (chance of recovery) is usually good.
The most common condition associated with MEN1 syndrome is hyperparathyroidism. Signs and symptoms of hyperparathyroidism (too much parathyroid hormone) include the following:
- Having a kidney stone.
- Feeling weak or very tired.
- Bone pain.
Other conditions associated with MEN1 syndrome and their common signs and symptoms are:
- Pituitary adenoma (headache, absence of menses during or after puberty, making breast milk for no known reason).
- Pancreatic neuroendocrine (islet cell) tumors (low blood sugar [weakness, loss of consciousness, or coma], abdominal pain, vomiting, and diarrhea).
- Malignant tumors of the adrenal glands, bronchi, thymus, fibrous tissue, or fat cells may also occur.
Children with primary hyperparathyroidism, tumors associated with MEN1 syndrome, or a family history of hypercalcemia or MEN1 syndrome may have genetic testing to check for a mutation (change) in the MEN1gene. Parents should receive genetic counseling (a discussion with a trained professional about the risk of genetic diseases) before genetic testing is done. Genetic counseling also includes a discussion of the risk of MEN1 syndrome for the child and other family members.
Children who are diagnosed with MEN1 syndrome are checked for signs of cancer starting at age 5 years and continuing for the rest of their life. Talk to your child's doctor about the tests and procedures needed to check for signs of cancer and how often they should be done.
MEN2A syndrome may cause medullary thyroid cancer, pheochromocytoma, or parathyroid gland disease.
MEN2A syndrome is also called Sipple syndrome. A diagnosis of MEN2A syndrome may be made when the patient or the patient's parents, brothers, sisters, or children have two or more of the following conditions:
- Medullary thyroid cancer (a cancer that forms in parafollicular C cells in the thyroid). Signs and symptoms of medullary thyroid cancer may include the following:
- A lump in the throat or neck.
- Trouble breathing.
- Trouble swallowing.
- Hoarseness.
- Pheochromocytoma (a tumor of the adrenal gland). Signs and symptoms of pheochromocytoma may include the following:
- High blood pressure.
- Pain in the abdomen or chest.
- A strong, fast, or irregular heartbeat.
- Headache.
- Heavy sweating for no known reason.
- Dizziness.
- Feeling shaky.
- Being irritable or nervous.
- Parathyroid gland disease (a benign tumor of the parathyroid gland or increase in the size of the parathyroid gland). Signs and symptoms of parathyroid gland disease may include the following:
- Hypercalcemia.
- Pain in the abdomen, side, or back that doesn't go away.
- Pain in the bones.
- A broken bone.
- A lump in the neck.
- Trouble speaking.
- Trouble swallowing.
- Familial medullary cancer of the thyroid is like MEN2A syndrome without pheochromocytoma or parathyroid tumors. A diagnosis of familial medullary cancer of the thyroid may be made when two or more family members have medullary thyroid cancer and no family members have parathyroid or adrenal gland problems. Signs and symptoms of medullary thyroid cancer may include the following:
- A lump in the throat or neck.
- Trouble breathing.
- Trouble swallowing.
- Hoarseness.
The prognosis is usually good.
A mutation in the RET gene is usually linked to medullary thyroid cancer in MEN2 syndrome. If a diagnosis of MEN2 syndrome is suspected for the child or a family member is diagnosed with MEN2 syndrome, the parents should receive genetic counseling before genetic testing is done for the child. Genetic counseling also includes a discussion of the risk of MEN2 syndrome for the child and other family members.
MEN2B syndrome causes several conditions.
Patients with MEN2B syndrome may have a slender body build with long, thin arms and legs. The lips may appear large and bumpy because of benign tumors in the mucous membranes. MEN2B syndrome may cause the following conditions:
- Medullary thyroid cancer (a fast-growing, aggressive cancer).
- Parathyroid hyperplasia.
- Adenoma.
- Pheochromocytoma.
- Nerve cell tumors in the mucous membranes or other places.
The prognosis for MEN2B syndrome is not as good as the prognosis for MEN1 syndrome and MEN2A syndrome because medullary thyroid cancer is a more aggressive cancer.
Children with MEN2A syndrome, MEN2B syndrome, or FMTC may need genetic testing.
A mutation in the RET gene is usually linked to medullary thyroid cancer in MEN2 syndrome. If a diagnosis of MEN2 syndrome is suspected for the child or a family member is diagnosed with MEN2 syndrome, the parents should receive genetic counseling before genetic testing is done for the child. Genetic counseling also includes a discussion of the risk of MEN2 syndrome for the child and other family members.
Tests used to diagnose and stage cancers related to MEN syndromes depend on the signs and symptoms and the patient's family history.
Tests are done to diagnose and stage cancer. After cancer is diagnosed, more tests are done to find out if cancer cells have spread to nearby areas or to other parts of the body. This process is called staging.
The following tests and procedures may be used:
- Physical exam and health history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient's health habits and past illnesses and treatments will also be taken.
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Blood hormone studies: A procedure in which a blood sample is checked to measure the amounts of certain hormones released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease in the organ or tissue that makes it. The blood may also be checked for high levels of the hormone calcitonin or parathyroid hormone (PTH).
- Genetic testing: A laboratory test in which cells or tissue are analyzed to look for changes in genes or chromosomes. These changes may be a sign that a person has or is at risk of having a specific disease or condition. A sample of blood is checked for the MEN1 gene to diagnose MEN1 syndrome and for the RET gene to diagnose MEN2 syndrome.
- Twenty-four-hour urine test: A procedure used to diagnose neuroendocrine tumors, such as pheochromocytoma. Urine is collected for 24 hours to measure the amounts of catecholamines in the urine. Substances caused by the breakdown of these catecholamines are also measured. An unusual (higher or lower than normal) amount of a substance can be a sign of disease in the organ or tissue that makes it. Higher than normal amounts may be a sign of pheochromocytoma.
- Ultrasound: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. The picture can be printed to be looked at later.
- MRI: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- CT scan: A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- PET scan: A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
- Thyroid scan: A small amount of a radioactive substance is swallowed or injected. The radioactive material collects in thyroid gland cells. A special camera linked to a computer detects the radiation given off and makes pictures that show how the thyroid looks and functions and whether the cancer has spread beyond the thyroid gland. If the amount of thyroid-stimulating hormone in the child's blood is low, a scan to make images of the thyroid may be done before surgery.
- Sestamibi scan: A type of radionuclide scan used to find an overactive parathyroid gland. A very small amount of a radioactive substance called technetium 99 is injected into a vein and travels through the bloodstream to the parathyroid gland. The radioactive substance will collect in the overactive gland and show up brightly on a special camera that detects radioactivity.
- Venous sampling for an overactive parathyroid gland: A procedure in which a sample of blood is taken from veins near the parathyroid glands. The sample is checked to measure the amount of parathyroid hormone released into the blood by each gland. Venous sampling may be done if blood tests show there is an overactive parathyroid gland but imaging tests don't show which one it is.
- Somatostatin receptor scintigraphy: A type of radionuclide scan that may be used to find tumors. A very small amount of radioactive octreotide (a hormone that attaches to tumors) is injected into a vein and travels through the blood. The radioactive octreotide attaches to the tumor and a special camera that detects radioactivity is used to show whether there are islet cell tumors in the pancreas. This procedure is also called octreotide scan and SRS.
- MIBG scan: A procedure used to find neuroendocrine tumors, such as pheochromocytoma. A very small amount of a substance called radioactive MIBG is injected into a vein and travels through the bloodstream. Neuroendocrine tumor cells take up the radioactive MIBG and are detected by a scanner. Scans may be taken over 1-3 days. An iodine solution may be given before or during the test to keep the thyroid gland from absorbing too much of the MIBG.
- Pentagastrin stimulation test: A test in which blood samples are checked to measure the amount of calcitonin in the blood. Calcium gluconate and pentagastrin are injected into the blood and then several blood samples are taken over the next 5 minutes. If the level of calcitonin in the blood increases, it may be a sign of medullary thyroid cancer.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer.
- Fine-needle aspiration (FNA): The removal of tissue using a thin needle.
- Surgical biopsy: The removal of tissue during surgery.
If cancer, such as medullary thyroid cancer, has formed, tests are done to find out if cancer cells have spread to nearby areas or to other parts of the body.
The process used to find out if cancer has spread to nearby areas or to other parts of the body is called staging. There is no standard system for staging childhood cancers linked to MEN syndromes. The results of the tests and procedures done to diagnose cancer are used to help make decisions about treatment.
Sometimes childhood MEN syndromes recur (come back) after treatment.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if medullary thyroid cancer spreads to the lung, the cancer cells in the lung are actually medullary thyroid cells. The disease is metastatic medullary thyroid cancer, not lung cancer.

